

By Габышев Дмитрий Николаевич (Own work) [CC0], via Wikimedia Commons
This post was inspired by one of my students who was studying from my upcoming “dreaded and feared" cardiac examination. She was completely honest with me when she said “I studied for 10 hours of cardiology and to be honest when I was done, I couldn’t tell you what I studied". I appreciated her honesty but I found it ironic because I had given them on the first day of class a blueprint on how to approach their studies. Most students approach studying in various levels of INEFFICIENCY and they think because they study for hours that makes it useful. IT IS BETTER TO STUDY FOR 3 HOURS EFFECTIVELY THAN TO STUDY FOR 20 HOURS INEFFECTIVELY. I’m not yelling at you in caps but I want those words to stick out to you so that if you take anything away from this blog, you take away those key points. I explained the rationale to this in the blog I posted last year called PATIENT CENTERED LEARNING but to get back to the topic, the purpose of this blog is to teach you how to approach arrhythmias simple and effective. Don’t believe me???? Keep reading this blog and I promise you that you will be an arrhythmia wizard at the end of it! But first things first, you know I am a big believer in understanding basic anatomy and physiology before going into pathophysiology and management because if you don’t UNDERSTAND how something is supposed to work, what went wrong won’t make sense and how to fix it also won’t make sense since the management usually reverses the pathophysiology.
BASIC ANATOMY
The heart has 2 upper chambers, the atria and 2 lower chambers the ventricles. That’s it!
BASIC PHYSIOLOGY
- WHO: the heart
- WHAT: does the heart have to do? Two simple functions. It has to 1) contract and 2) relax. That’s it!
- WHEN: hopefully all the time (because if your heart stops, you won’t be able to finish this blog).
- WHERE: I’m sure you know where the heart is before reading this blog so let’s move onto the why…
- WHY: The heart 1) contracts to send blood to the body (so you can stay alive to read the rest of the blog) and 2) it has to relax to fill with blood to start the process of contraction all over again. That’s it!
- HOW: The ventricles first fill passively with blood when the AV valves open by sheer gravity. At the very end of ventricular diastole (relaxation) the atria contracts the remaining amount of blood into the ventricle. The electrical conduction system of the heart is wired to allow the heart to contract effectively and then relax to allow the process to start all over again. If you understand the electrical conduction system, you can scroll down straight to the section of the golden rules of arrhythmias (but I recommend reading the whole thing so everything makes sense).
ELECTRICAL CONDUCTION SYSTEM
- Sinoatrial node: the primary pacemaker of the heart (located in the upper right atrium). The intrinsic rate of the SA node is 60-100 beats per minute.
- Atrioventricular node: has 3 functions: 1) it briefly delays the impulse it receives from the SA node. Why?? Because you don’t want your atria and ventricles to contract at the same time (the atria needs to contract the remaining blood into the ventricle before the ventricles contract). By briefly delaying the impulse, the AV node accomplishes this. 2) Its second job is to be a backup pacemaker of the heart. If the SA node fails to fire, it can take over as a backup pacemaker to keep you alive long enough to finish reading this blog. The intrinsic rate of the AV node is 40-60 beats per minute. The lower part of the atria surrounding the AV node, the AV node and the surrounding cells of the bundle of HIS are collectively known as the AV JUNCTION. Therefore, we often refer to rhythms originating from this area as “junctional." Once the impulse is briefly delayed, the Bundle of HIS rapidly sends the impulse to the ventricles to ensure uniform ventricular contraction.
GOLDEN RULES TO TREAT ARRHYTHMIAS
GOLDEN RULE #1
Simply put, ALL ARRHYTHMIAS CAN ONLY COME FROM 3 PLACES!
1) the atria 2) the AV junction or the 3) ventricles.
Atrial arrhythmias: are characterized by the presence of a P wave (since P waves reflect atrial depolarization and hopefully atrial contraction). Therefore atrial rhythms have P waves present (or flutter waves in atrial flutter and fibrillatory waves in atrial fibrillation) and are classically associated with a narrow QRS complex (reflecting normal conduction of the impulse to the ventricles). The exceptions to this rule are 1) if the beat was aberrantly conducted or 2) a bundle branch blocks is present. In those situations, the QRS will be wide (but that is for another blog and time). Take home point: In general atrial arrhythmias (expect flutter and fib) are associated with the presence of a P wave and a narrow QRS complex. P waves of SA origin are usually positive in leads I, II and avF on an ECG and negative in AVR (they can be positive, negative or biphasic in other leads).
Junctional rhythms: are characterized by the absence of P waves (since the origin of the impulse is the AV junction, it sends the impulse retrograde to the atria at the same time it sends the impulse to the ventricles so the P wave becomes “hidden" in the QRS). If P waves are present they MUST be inverted (negative) P waves in leads I, II and/or avF (reflecting retrograde atrial depolarization from the floor of the atrium to the top instead of the normal way which is from the top of atria to the floor of atria). Since there is normal conduction, the QRS is expected to be narrow (unless the beat was aberrantly conducted or bundle branch blocks are present and then the QRS will be wide). Take home point: Junctional rhythms are associated with no P wave (or inverted P waves if present) and are expected to have a narrow QRS complex.
Ventricular rhythms are always abnormal. Because idioventricular rhythms don’t use the normal, efficient electrical conduction system as its way to conduct the impulse throughout the ventricles, it inefficiently sends the impulse from cell to cell to cell (which takes a longer time, resulting in a wide QRS).
This is adapted from the AHA guidelines:
If the rhythm you are evaluating is a tachyarrhythmia, go to Golden Rule 2.
If the rhythm you are evaluating is a bradyarrhythmia, then go to Golden Rule 3
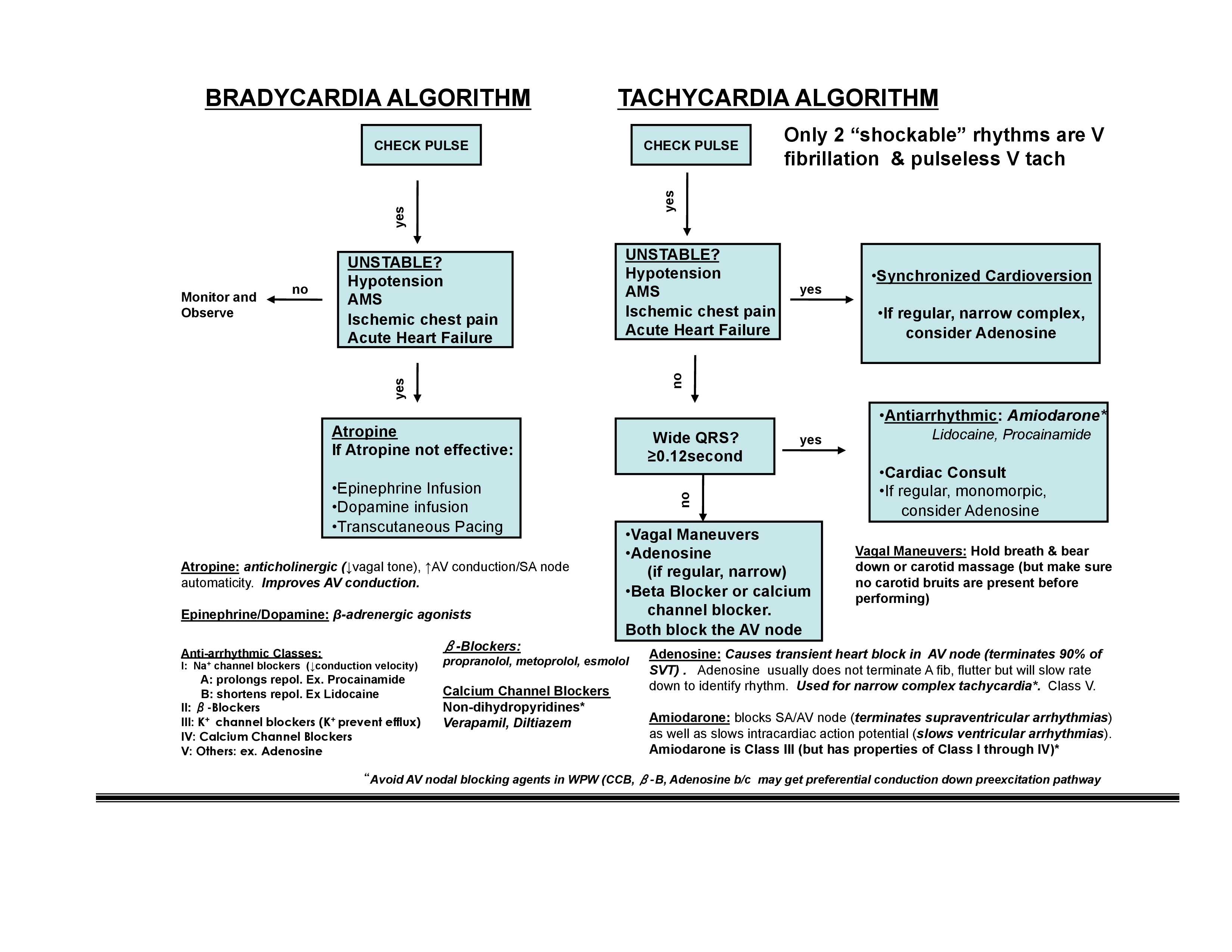
GOLDEN RULE #2 FOLLOW THE TACHYCARDIA ALGORITHM!!!!!
As I sat with another student during this same study session, I gave her this golden rule and it was amusing to watch her say she understood it but then went right back to not using the golden rules, leading her to inadvertently give me the wrong answer. I would tease her when she got the answer wrong and ask her “did you follow the golden rule?" she would admittedly say no and then when she did she would get the right answer. At the end of the session she was able to answer the management in less than 1 minute because she began to follow the golden rule, so I forbid you to read further if you don’t promise me that you will follow these golden rules.
STEP 1: check the patient to see if they have a pulse. If there is no pulse, then this algorithm is not used. No pulse = cardiac arrest!!!! Without a pulse there is no perfusion so you have to manually pump the heart (via manual compressions during CPR) until you can fix whatever caused the cardiac arrest. There are 4 types of cardiac arrest: 2 rhythms that are “shockable" via unsynchronized cardioversion aka defibrillation and 2 “nonshockable" rhythms. Since they all have no pulse, all 4 require CPR until a pulse can be reestablished (hopefully).
2 shockable rhythms with defibrillation (aka unsynchronized cardioversion) are: 1) Ventricular fibrillation (who would have thought right?) and 2) pulseless Ventricular tachycardia. Why pulseless V tach?? Because the natural downward progression of ventricular tachycardia is for ventricular tachycardia with a rapid pulse to deteriorate into ventricular tachycardia without a pulse and eventually into ventricular fibrillation. Since ventricular tachycardia without a pulse is essentially the pathway into ventricular fibrillation, they are treated the same. Why give them a shock?? The idea is that these rhythms perpetuate due to some of the cells in the relative refractory period and some cells in the absolute refractory period. Defibrillation puts all the cardiac cells in the absolute refractory period SIMULTANEOUSLY to terminate the perpetuation of the dangerous rhythm and allows the SA node to take back its rightful ownership as the dominant pacemaker of the heart.
2 nonshockable cardiac arrest rhythms: pulseless electrical activity and asystole.
STEP 2: If a pulse is present, then check to see if the patient is stable or unstable.
- If the patient has unstable tachycardia, then the management of choice is SYNCHRONIZED cardioversion. Not to be confused with unsynchronized cardioversion (defibrillation) described above. The reason it must be synchronized (the shock must be delivered on the R wave to prevent giving the shock on the relative refractory period of the T wave). Giving the shock on the T wave can cause ventricular fibrillation to occur as a result of administering the shock. Ventricular fibrillation that occurs when an ectopic beat occurs on the relative refractory period of the T wave is known as the “R on T" phenomenon.
- If the patient has stable tachycardia then go to step 3
STEP 3: is the QRS narrow or wide? The reason you want to know if the QRS is narrow or wide is to determine where the problem is likely originating from. If the QRS is narrow, then the impulse is supraventricular and is conducted normally to the ventricles. Knowing this is critical in determining which is the best medication to use if vagal maneuvers don’t work. If the QRS is wide, it means the rhythm is ventricular in origin (or aberrantly conducted) which also changes the medications you would use.
- Narrow regular complex tachycardia (especially if thought to SVT or AV nodal reentry): Adenosine, Beta blockers or calcium channel blockers. Adenosine is the first line management of narrow, regular complex tachycardia thought to be due to AV nodal reentry because AV nodal reentry is the most common cause of supraventricular tachycardias (SVT). In people with a normal pathway in the AV node and a second, abnormal pathway WITHIN the AV node, a premature atrial impulse will continue to go around in circles in the AV node repeatedly perpetuating that original impulse multiple times into the ventricles and the atria (causing AV nodal reentry tachycardias that can present as SVT). AV nodal blockers such as adenosine breaks the circuit, therefore terminating the arrhythmia. Adenosine has a really short half life (seconds) which is long enough to break the rhythm. Beta blockers and calcium channel blockers also block the AV node and can terminate these rhythms as well.
- Wide complex tachycardia: antiarrhythmics such as Amiodarone are first line management. Why antiarrhythmics and not primary AV node blockers? Because wide complexes indicate a ventricular origin of the tachycardia or aberrantly conducted rhythm in the ventricles, so AV nodal blockers won’t be helpful because the problem is below the AV junction. Other antiarrhythmics (such as procainamide and lidocaine) may also be used in specific situations. An indication to the use of lidocaine is in patients who are having an MI presenting with wide complex tachycardias because lidocaine has been shown to reduce arrhythmias effectively in ischemic cardiac tissue.
There are 3 main exceptions to rule 3:
Exception 1: Atrial flutter and atrial fibrillation, skip adenosine and go straight to calcium channel blockers or beta blockers. Why are these exceptions to the rule? Because in atrial fibrillation, the problem are multiple ectopic foci firing in the atria. If you transiently block the AV node in atrial fibrillation it will temporarily slow down the rhythm (so adenosine may be used for diagnostic purposes to slow down the rhythm long enough to see what underlying rhythm is present) but as soon as the medication wears off, the ectopic foci that are firing through this process will speed up the ventricular rate again and you are back to square one! Beta blockers and calcium channel blockers will continue to reduce the impulses that make it through the ventricle. They are still in atrial fibrillation, but the ventricular rate will be slowed down with the calcium channel blockers or the beta blockers. That’s why we call that “rate control" instead of rhythm control. In atrial flutter, only one focus is firing but the same rules apply as I just discussed for atrial fibrillation.
Exception 2: treat the underlying cause in patients with sinus tachycardia and the rhythm usually resolves.
Exception 3: Procainamide is the preferred antiarrhythmic agent for WPW. For other rhythms thought to occur because of a second, abnormal pathway OUTSIDE the AV node (known as AV reciprocating tachycardias), blocking the AV node with AV nodal blockers may cause preferential conduction down the abnormal, fast pathway. By blocking the inhibitory effect of the AV node, AV nodal blockers may worsen the arrhythmias, so procainamide (or other antiarrhythmics) are preferred. The most common type of AV reciprocating tachycardias is Wolff-Parkinson White in which the abnormal pathway (Kent Bundle) is the issue. Procainamide is preferred in the management of WPW over the antiarrhythmics.
All you have to do is identify the rhythm you see and plug it into the algorithm and then it’s easy to know what to do!
Don't believe me??? Try these 3 cases:
Case 1: the nurse calls you to the floor to assess a patient. The telemetry strip shows the following:

You walk into the room the patient is unresponsive, hypotensive and there is no palpable pulse present. What do you do??
Step 1: check pulse. Since the patient has no pulse, he is in cardiac arrest. The management of pulseless ventricular tachycardia is to start CPR and compressions and unsynchronized cardioversion (defibrillation). If you got that right, you followed the rule.
Case 2: the nurse calls you to the floor to assess a patient. The telemetry strip shows the following:
You walk into the room and the patient is anxious, having palpitations and mild shortness of breath. The blood pressure is 190/110 with a rapid pulse rate.
What do you do?
Step 1: check pulse. The patient has a pulse
Step 2: stable vs. unstable: the patient is hypertensive and responsive. They are symptomatic but stable.
Step 3: Is the QRS narrow or wide? There is a regular rhythm with a wide QRS so therefore, amiodarone is the preferred agent for a stable wide complex tachycardia. If you got that right, you followed the rule.
Case 3: the nurse calls you to the floor to assess a patient. The telemetry strip shows the following:
You walk into the room and the patient is lethargic, hypotensive, diaphoretic but there is a palpable rapid, weak pulse. What do you do?
Step 1: Check pulse. The patient has a rapid but palpable pulse.
Step 2 is the patient stable or unstable? The patient is unstable based on the physical exam findings
Based on the unstable tachycardia with a pulse, the management is to prepare for synchronized cardioversion to stabilize the patient. If you got that right, you followed the rule.
Notice the monitor showed the same exact rhythm in all 3 cases but there are three very different approaches to the management. TREAT THE PATIENT NOT THE ECG! If you plug in any tachyarrhythmias to the rule with the notable exceptions given to you the rule holds true in terms of which medicine to use. Unstable atrial flutter, unstable multifocal atrial tachycardia, unstable atrial fibrillation or any other unstable tachyarrhythmias with a pulse, synchronized cardioversion is the management of choice as per the AHA guideline. So all you do is plug the rhythm you see into the algorithm and assess the patient.
GOLDEN RULE #3 FOLLOW THE BRADYCARDIA ALGORITHM!!!!!
This algorithm has one step less than the tachyarrhythmia algorithm.
Step 1: check the patient to see if the have a pulse. If there is no pulse, No pulse = cardiac arrest!!!!
Step 2: If a pulse is present, then check to see if the patient is stable or unstable.
- If the patient has unstable, symptomatic bradycardia, then the first line management is atropine. Atropine is an anticholinergic drug that indirectly increases sympathetic tone by blocking parasympathetic tone (remember that acetylcholine is the chief neurotransmitter of the parasympathetic system, so by blocking acetylcholine, the sympathetic tone increases). Other medications used in the management of unstable, symptomatic bradycardia are epinephrine or dopamine (which directly stimulates the sympathetic system and increased the rate of both SA node and AV node firing, resulting in an increased heart rate). Other modalities that can be used if medical management is not effective is transcutaneous pacing (or permanent pacing) for a more definitive management.
- If the patient has stable bradycardia, then no immediate medical management is needed. The patient may be observed, cardiac consult or referral may be needed but you don’t need to medically manage immediately.
The exception to the bradycardia rule is third degree heart block. Temporary cardiac pacing is the preferred management. You can administer atropine or a dopamine infusion. If the atropine or dopamine works, then the block is due to abnormal AV node conduction. Atropine is unlikely to work in third degree block below the bundle of HIS so temporary pacing will be needed until the rhythm resolves or a more definitive management can take place.
If you understand and follow these three golden rules, you will know how to effectively manage all the patients not only on the PANCE but in clinical practice! All my best!
Dwayne A. Williams is the author of Pance Prep Pearls, PANCE and PANRE question book and the Ultimate Medical Mnemonic Comic Book. He is also the maker of the FlipMed medical app.